








Introduction
Framing the question simply as “who cares more—men or women” risks overlooking the structural and cultural forces that shape care work. Care labour is deeply ingrained in social norms and has historically been feminised. “Although criticisms on care responsibilities are usually centred around women’s disproportionate burdens, the other side of this imbalance lies in the limited participation of men in caregiving and domestic work. The persistence of gendered norms that assign care to women does not only reinforce the unequal division of labour within households, it also undermines the effectiveness of workplace policies, social programmes, and economic reforms aimed at promoting gender equality.
However, during the COVID-19 pandemic, there was a significant increase in men reporting housework and family responsibilities for labour force withdrawal. This shift raises a critical question: was the pandemic able to initiate more transformative and enduring changes in household care arrangements or did it merely produce a temporary adjustment in men’s involvement in care responsibilities? This article aims to situate these rises alongside pandemic and post-pandemic labour trends to provide insights into whether men’s participation in care reflects a substantial shift or remains only supplementary to women’s primary caregiving roles.
Men in women’s field: dual earner but not dual carer
“…women have gone into the workforce, that was the revolution, but the workplace they go into and the men they come home to have changed less rapidly, or not at all.”1
The quote from Arlie Russell Hochschild reveals the contrasting paths of the gender revolution: while women have increasingly entered and succeeded in domains historically coded as masculinity, namely paid employment and professional careers, men’s participation in care— traditionally coded as feminine—remains partial and uneven, reflecting an asymmetrical transformation of household and social responsibilities. The revolution in women’s roles has been hampered by the inequivalent revolution in men’s roles in terms of caregiving/household chores.
In households, there are preferred family models that are widely practised, such as partnership model where both parents do paid work and share care responsibilities equally, disproportionate (female) model in which both partners work but women additionally takes care of the house and children, and the traditional patriarchal model where the breadwinner is the father, while the mother does not do paid work and fully takes care of the house and children2. The dual-earner or universal breadwinner model have been the most prevalent in recent decades, driven by economic necessities and broader strides toward gender equality in the workforce.
However, these shifts in employment patterns have not been accompanied by a corresponding reorganisation of care responsibilities within households. The universal breadwinner model often does not seek to increase men’s contribution to unpaid care, but rather reduce women’s caregiving burden to free up their time to participate in labour market3. While, in theory, the model aims to redistribute care responsibilities to the state or the market, there remains a portion of care activities that can only be provided by women, resulting in the “double burden” of managing both full-time employment and unpaid caregiving4.
Covid-19, care and men
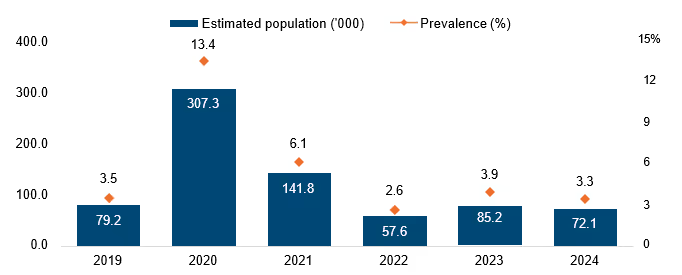
The COVID-19 pandemic provides useful data for examining changes in care arrangement. It disrupted conventional divisions of paid and unpaid work through lockdowns, which resulted in the implementation of full-time remote work, and the closure of schools and childcare centres. These disruptions compelled households to renegotiate care responsibilities and rendered unpaid care more visible in statistical measurement and labour force data. Cross-national surveys covering women and men in 47 countries indicated that men undertook more hands-on care during the pandemic than at any other point in recent history5. In Malaysia, evidence similarly suggests an increase in men’s involvement in domestic and household work during 2020 (Figure 1). Data from the Department of Statistics Malaysia (DOSM) shows a sharp rise in men citing housework and family responsibilities as the main reasons for their exclusion in the labour force. However, this sentiment had declined post-pandemic, suggesting that the shift in gender roles attributed to household care was temporary. This pattern points out how labour market disruptions are intersected with care demands rather than signalling a fundamental redistribution of care responsibilities.
The rise in men citing housework and family responsibilities during the pandemic raises the question of whether this reflected a shift toward egalitarian care arrangements or merely a temporary, crisis-driven adjustment. Although labour market disruptions formed a broader backdrop of the pandemic, attributing men’s increased care involvement solely to unemployment risks had overlooked the constraining force of unpaid care itself. In Malaysia, men who exited the labour force during this period reported housework and family responsibilities as their primary reasons, indicating that care demands had impacted labour supply decisions. However, as economic activity resumed and childcare centres reopened, men’s participation in unpaid care begin to recede. Women’s care responsibilities, in contrast, remained elevated beyond the crisis period, leaving gendered division of unpaid care largely intact.
Figure 1: Housework and family responsibilities as reasons for not seeking work cited by men
Economic crises, including the 2008 financial downturn and the COVID-19 pandemic, revealed a recurring pattern as attention is primarily given to the impacted male-dominated sectors, such as construction and manufacturing6. However, the pandemic’s impact on women-dominated sectors remained obscure and unexplored, making it unknown whether women’s employment prospects would be more affected than men’s during the financial crisis7.
Women are over-represented in-service and informal industries which puts them in higher risk of job losses during the lockdown. At the same time, they are also over-represented in frontline responders’ occupations deemed critical to the pandemic response8. In Malaysia, women constitute the majority of the health workforce, including 96% of nurses9. Beyond clinical roles, women also make up a large share of hospital support staffs — such as cleaners, sanitation workers and caterers who are essential to healthcare operations, further amplifying their increased exposure and workload during the crisis10.
These women-dominated sectors are often classified as “essential,” placing workers at greater risk of virus transmission, morbidity, and mortality due to the less-digital and hands-on nature of the work. At the same time, the rise in men citing housework and family responsibilities as their primary reasons for being outside the labour force in Malaysia challenges the broader notion that men’s labour force exit during the pandemic was driven solely by lockdowns or unemployment.
Evidence from a Malaysian COVID-19 study demonstrates that men’s share of childcare increases when women contribute a larger proportion of household income11. These patterns suggested that women’s sustained participation in public-facing roles during the pandemic had renegotiated the contribution of household care between men and women, reflecting the temporary increase in men ‘s withdrawal from labour force due to family responsibilities.
In addition to experiencing disproportionate job losses and heightened exposure to frontline risks, women maintained primary responsibility for caregiving tasks—including unpaid domestic work, childcare, and eldercare—which analysts describe as ‘she-cession’, alluding to the economic consequences of COVID-19 towards women12. Ironically, the framing of post-crisis strategies to prioritise “man-covery”13 are intensified compared to women-dominated industries, leaving caregiving responsibilities remained undiscussed and largely borne by women. The different treatment of gender in household and labour force risks entrenching unequal division of care in the long run.
Care division during the pandemic
Studies consistently show that men and women experienced the COVID-19 pandemic differently. These differences are shaped by both preconceived gender norms and employment arrangements14. In Malaysia, KRI’s pre-pandemic time-use survey found that women devoted a larger share of their time to unpaid care and domestic work averaging from 3.6 hours per day compared to men’s 2.2 hours, despite women’s near-equal participation in paid employment15.
Building on earlier observations of men’s increased engagement with domestic responsibilities, questions remain unaddressed about how these changes translated into equal division of care within households during the pandemic.
A Malaysian-based online survey examined the time spent (weekly hours) between spouses with their children on paid work, housework, and childcare from 467 couples during the pandemic. According to the findings, women reported spending an average of 18.6 hours per week on housework compared to men who allocated 11.7 hours, and 22.4 hours per week on childcare in contrast to 14.5 hours by men16,17. These figures suggest that pandemic had intensified women’s care contributions by layering new tasks (e.g. supervising remote education and managing daily household routines) onto pre-pandemic obligations.
A qualitative interview was conducted during two lockdown periods in Poland which examined how work-from-home (WFH) arrangements shaped fathers’ narratives about care and family life. While WFH heightened fathers’ awareness of household demands and emerging care responsibilities, their involvement often remained episodic and secondary to paid work, occurring primarily during “free time”18. In contrast, mothers experienced care as an ongoing responsibility, combining paid employment with domestic and caregiving tasks throughout the day19. This pattern echoes the qualitative studies of Malaysian households, where most women reported performing housework largely on their own, while most men perceived it as a shared responsibility20. Men’s contributions also often took the form of backups or “chipping in” when needed21.
It is evident that women’s expanding roles and hyper-independence perform unpaid care highlights the need to recognise the gendered impacts and the evolving position of women in both society and the economy, alongside the continued stagnation of men’s participation in caregiving.
Calling for men’s involvement and care to be gender inclusive
KRI conducted a survey in collaboration with Persatuan Suri Rumah Rahmah (SRR) among housewives, asking what forms of support could increase their husbands’ or male family members’ participation in caregiving. The most commonly cited measure, supported by 55.9% of respondents, was the implementation of programmes that normalise and promote shared family roles22. This includes public awareness campaigns, affirmative media representations of caregiving fathers, and visibility of male role models who actively engage in domestic and care responsibilities23. This highlights the need to move beyond framing care as women centric and to focus on men’s limited participation in caregiving. Labour market care policies often speak primarily to women, treating care as a tool to encourage their labour force participation while leaving men largely out of the conversation24.
Without explicitly calling on men to assume greater caregiving responsibilities, stereotype gender norms associated with care would less likely be dismantled. Family-friendly and flexible work initiatives must therefore move beyond helping women “manage” care and actively promote men’s equal participation. Expanding access to adequate paternity leave and encouraging men’s uptake of such leave, alongside their active involvement in caregiving, are critical steps in challenging gendered expectations and normalising shared responsibility in households, communities, and societies.
Conclusion
While the COVID-19 pandemic saw men performing more hands-on caregiving roles, their contribution was merely episodic and did not fundamentally redistribute care responsibilities. Care is continuous and relational, rather than a temporary market problem or a commodity that can be adjusted through short-term shocks. It unfolds across the life course within households and societies, sustained by everyday practices of responsibility and obligation.
Precisely because care is relational and enduring, promoting men’s continuous engagement in caregiving cannot rely solely on temporary disruptions or short-term shifts in working arrangements. Instead, policies and social norms must actively encourage men’s long-term participation in unpaid care—through workplace flexibility for fathers, non-transferable parental leave, and cultural shifts that redefine caregiving as compatible with masculinity. Recognising and supporting women as the primary contributor of caregiving must therefore go hand in hand with structural integration of men into caregiving roles to reposition care as a shared social responsibility rather than a residual burden borne primarily by women.





